
By Robert D. Levine, DDS
Director of Laser Dentistry, Assistant Professor – Clinical Dentistry. Arizona School of Dentistry & Oral Health: Mesa, Arizona
Introduction
Oral Irritation Fibroma is a common, benign, scar-like reaction to persistent longstanding irritation in the mouth. It is also known as traumatic fibroma, focal fibrous hyperplasia, fibrous nodule or oral polyp. It is most commonly seen in older adults but can occur at any age and affects one to two percent of all adults. It is usually due to chronic irritation such as biting of the cheek or lip, rubbing of skin against a rough tooth or dentures and other oral prostheses [1-3].
Oral fibroma presents as a firm, smooth, rounded tumor (lump). It is typically clearer than the surrounding tissues but the same color as the rest of the mouth lining. It is sometimes more pale or, if it has bled, may appear to be a darker color. It is well demarcated and covered with ordinary mucosa (no erosion or hyperkeratosis) and the surface may be ulcerated due to trauma or become rough and scaly. Though it is generally dome-shaped, it may also be pedunculated. Additionally, if it has developed under a denture it may be flat with a leaf-like shape [1].
The most common location for an oral irritation fibroma is on the inside of the cheek where the upper and lower teeth meet. Other common sites include the sides of the tongue, gums and inside the lower lip. Apart from the feel and appearance, oral fibromas do not cause any symptoms. Oral fibromas develop over weeks or months to reach a maximum size typically about 1 cm in diameter, but can sometimes be larger. Oral fibroma most often is a solitary lesion. When there are many lesions, associated diagnoses need to be considered including tuberous sclerosis, Cowden syndrome, familial fibromatosis and fibrotic papillary hyperplasia of the palate. Oral fibromas do not develop into oral cancer [1].
Surgical Solution
Diagnosis and treatment of a fibroma requires excision with one to two millimeter mucosal “safety” margins. It may recur after surgery if the source of irritation continues. It is therefore also important to manage the source of the irritation but it should be noted that the recurrence rate is very low [2].
As a benign tumor, fibromas may grow aggressively and oral fibromas do not disappear without treatment. Therefore, rapid identification and surgery are recommended. Utilizing 10.6 micrometer wavelength CO2 surgical laser technology for fibroma removal minimizes potential recurrence and improves the cosmetic outcome [2].

Initial Findings
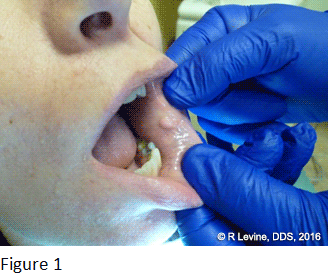
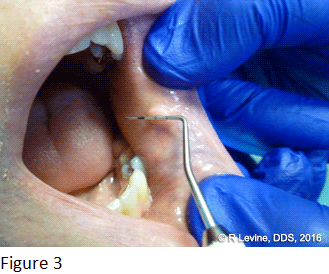
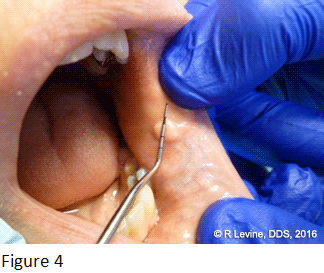
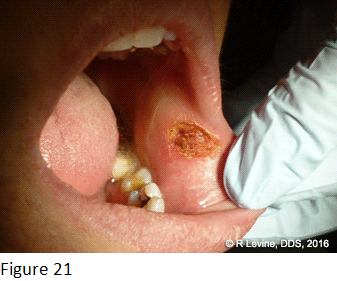
This particular patient presented with an 8 mm x 8 mm circumscribed lesion attached to lower inner labial mucosa (Figures 1-4). The patient stated that the lesion had been present for about five years and was slowly increasing in size. The patient requested that it be removed and the method chosen for removal was the use of the LightScalpel CO2 Dental Surgical Laser in SuperPulse(char free) mode.




Procedure – LightScalpel Laser Excision
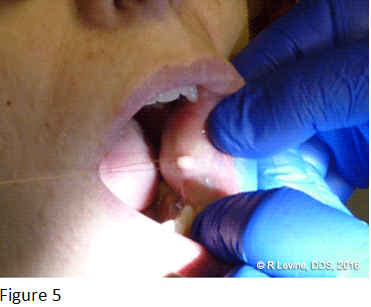
Local anesthesia was administered by local infiltration and an incision was made with the laser in focused mode with nozzle to tissue distance in 1-2 mm range. Tension needed to be placed on the mass during the procedure to allow for clean and uniform removal; this was done by threading a suture through it (Figure 5).


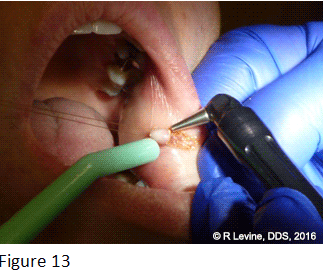
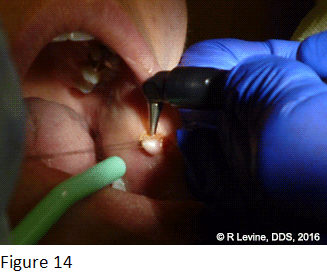
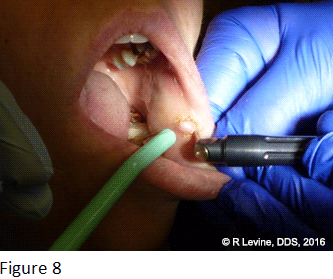
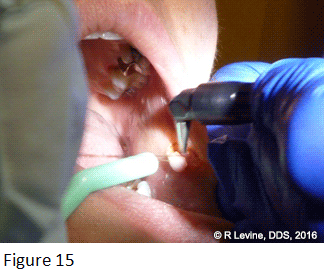
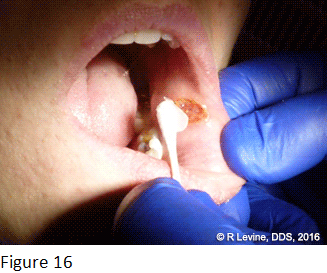
The LightScalpel laser was set to 2.9 Watts average power in SuperPulse mode (Repeat Pulse setting F2-5 at 4 Watts SP). Tipless angled handpiece was utilized at 1-2 mm distance from nozzle to tissue ensures 0.25 mm focal spot size on the tissue (designed for cutting, incising and excising). The growth is gently pulled outward to provide tension using the ends of the suture while excision of the mass was performed with the LightScalpel laser handpiece (Figures 6-15). If persistent oozing is encountered during the procedure, pressure should be applied for several minutes using moist gauze and additional hemostasis provided if necessary (Figure 16) [2].

Post Op
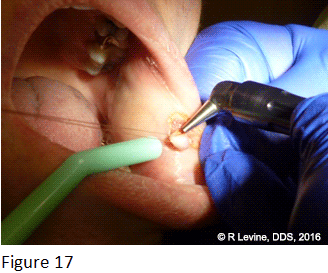
This procedure was cleanly performed without need for sutures. The growth was neatly excised with the laser providing coagulation of the area as the incision was being made with minimal need for suction (Figure 17). Note the lack of blood and cleanly cut area in figures 18-21.Topical antibiotic and vitamin “E” gel were prescribed to be applied directly to the area to aid in recovery. The patient reported minimal discomfort during or after the procedure. Recovery was uneventful and with a great aesthetic outcome.

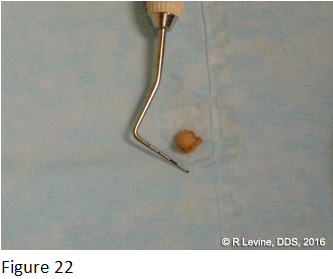
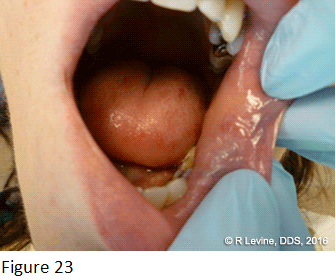
The excised fibroma specimen was sent for a histopathological analysis (Figure 22) and was indeed determined to be a non-cancerous fibroma in the returned report. In figure 23, the area is shown two weeks post procedure: note the clean healing on the lower labial mucosa. The use of a CO2 surgical laser is an excellent way to ensure the removal of the fibroma and lower the chance of recurrence. It makes the procedure faster and cleaner with less discomfort for the patient.
Summary
The LightScalpel 10.6 µm CO2 dental surgical laser with the LightScalpel angled tipless handpiece is an invaluable tool for dentists who perform soft tissue surgical procedures for their clients. The advantages include a more comfortable and, according to feedback from patients, less painful experience which should ultimately lead to positive reviews of work performed. The ability to do more procedures utilizing fewer resources leads to the opportunity for a dental surgeon to serve more patients which benefits both patients and practice! This absolutely provides an advantage for dental surgeon’s professional growth and development as well as the financial success of the practice.
| See the LightScalpel laser in action Watch Laser Surgery Videos | Learn more about soft-tissue dental laser surgery Soft-Tissue Laser Dentistry |
References
- DermNet New Zealand Trust (Corporate Author). Oral (irritated) fibroma (May) 2010 Page URL: http://www.dermnetnz.org/site-age-specific/oral-fibroma.html
- Sawisch, TJ. Ablation/Vaporization Techniques and Procedures – Clinical Scenarios. Principles and Practices of Laser Dentistry. Convissar, R. 2011: pp. 107-108
- Namour, S. Atlas of Current Oral Laser Surgery 2011: pp. 27-36


